2021 FSA Posters
P034: SUCCINYLCHOLINE USAGE IN THE PEDIATRIC POPULATION AT THE UNIVERSITY OF FLORIDA- A RETROSPECTIVE ANALYSIS.
Lida Esfandiary, MD; Taranjit Sangari, MD; UFL
Introduction: Pediatric laryngospasm is an airway emergency as it can lead to complete airway obstruction with fatal ramifications. It is considered standard of care to begin with non-invasive measures such as positive pressure ventilation, jaw thrust and Larson’s maneuver (pressure on the body of mandible anterior to the mastoid process) to facilitate airway exchange. In situations with failed conservative management, succinylcholine is a well-established treatment for laryngospasm. We present a retrospective analysis on the usage of succinylcholine at our institution in hopes to shed light on high risk cases with increased laryngospasm prevalence.
Methods: A retrospective chart review was conducted on pediatric patients undergoing surgery at the University of Florida from July 2019 – July 2020. These cases were further divided to evaluate the number of times succinylcholine was documented for emergent or non-emergent use. The emergent use of succinylcholine was then stratified to examine the specialties (otolaryngology/ENT, orthopedics, urology, and pediatric surgery) along with the timing in anesthesia (induction, maintenance and emergence) for laryngospasm treatment.
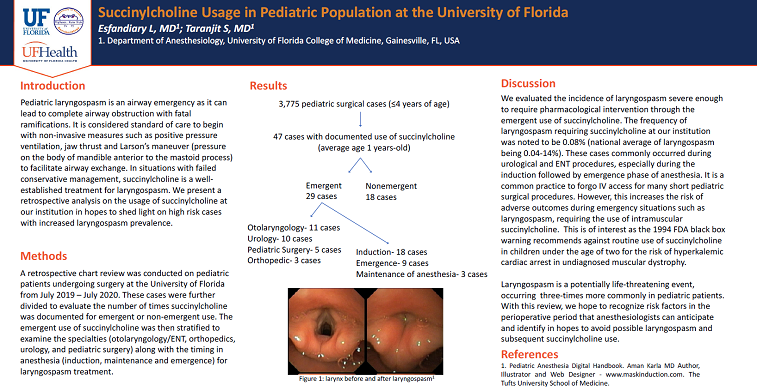
Results: There were 3,775 pediatric (≤4 years of age) surgical cases performed at our institution in one year. 47 of the 3,775 cases (average age: 1-years-old) had documented use of succinylcholine. These 47 cases were then stratified into emergent (n=29) and non-emergent (n=18) cases. An analysis of the type of surgical cases and timing of succinylcholine administration was conducted. This revealed that otolaryngology (n=11) followed by urology (n=10) had the most frequent succinylcholine administration with pediatric surgery (n=5) and orthopedic (n=3) cases having the least use. The same analysis was again performed on the timing of administration which elucidated that emergent cases received succinylcholine commonly during induction (n=18) followed by emergence (n=9) and maintenance of anesthesia (n=3).
Discussion: In our study, we evaluated the incidence of laryngospasm severe enough to require pharmacological intervention through the emergent use of succinylcholine. The frequency of laryngospasm requiring succinylcholine at our institution was noted to be 0.08% (national average of laryngospasm being 0.04-14%). These cases commonly occurred during urological and ENT procedures, especially during the induction followed by emergence phase of anesthesia. It is a common practice to forgo IV access for many short pediatric surgical procedures. However, this increases the risk of adverse outcomes during emergency situations such as laryngospasm which then requires the use of intramuscular succinylcholine. This is of interest as the 1994 FDA black box warning recommends against routine use of succinylcholine in children under the age of two for the risk of hyperkalemic cardiac arrest in undiagnosed muscular dystrophy.
Conclusions: Laryngospasm is a potentially life-threatening event that occurs three-times more commonly in pediatric than adult patients. With this review, we hope to recognize risk factors in the perioperative period that anesthesiologists can anticipate and identify in hopes to avoid possible laryngospasm and subsequent succinylcholine use. Additional studies with larger cohorts must be conducted to confirm our findings.